Surgical therapy:
Goals
The primary initial goal in the treatment of traumatic amputations is to evaluate the suitability of the amputated part for replantation. Amputations of the thumb, multiple fingers, the hand at the level of the wrist or distal forearm, and the upper extremity above the elbow should be evaluated for replantation because patients can benefit functionally from replantation of these appendages even if function of the part is less than optimal.
Often, replantation at these levels can achieve good functional outcomes. Replanted single fingers can be stiff and impede the opposition of other fingers to the thumb and overall hand function. Replanted single-finger amputations can achieve better range of motion when the level is distal to the insertion of the flexor digitorum superficialis (May, 1982).
Single-finger replantation can be considered when patients have injuries to other fingers of the same hand; all of these injuries require splint immobilization and rehabilitation that impedes immediate return to work. Accordingly, single-finger replantation can be considered in special circumstances. The surgeon must not become absorbed in the technical challenge of the replantation and neglect the other associated injuries because poorer outcomes and greater financial cost (due to lost wages and cost of hospitalization and therapy) can result.
In performing an amputation, it is important to preserve functional length. For example, an above-elbow arm amputation should be replanted to provide the patient with a functional elbow on which a prosthesis can be fitted, resulting in better function than an above-elbow prosthesis. Durable coverage at the end of an amputation is critical to the function of an amputation. This may necessitate the use of a local flap. Preservation of sensibility on the amputation stump can optimize the usefulness of the remaining appendage.
Sometimes, local flaps can be used to bring sensate tissue to the stump tip. It is important to minimize the risk of painful neuroma formation at the amputation stump and to prevent joint contractures in the treatment of amputations. Some local flaps can pose a risk of joint contracture to the involved finger and adjacent fingers. Use of the delayed groin flap can risk elbow and shoulder joint contractures. Other critical objectives in the treatment of amputations are early return to work and fitting with a prosthesis when possible.
Digital amputations
In performing digital amputations, provide a mobile, stable, painless stump with the least interference from remaining tendon and joint function to provide the most useful amputation stump. The remaining viable skin is conserved because it may be needed to provide durable soft tissue coverage for the amputation stump. When possible, use volar skin for stump coverage because it provides skin that is thicker and more sensate than dorsal skin (Omer, 1978).
There are several local options for tissue rearrangement of volar skin over the amputation stump. These include fillet flaps, volar V-Y flaps, bilateral V-Y flaps, and homodigital island flaps (Wilhelmi, 2002). Dog ears in the acute traumatic amputation should often be left to eliminate tension and to prevent compromising blood flow to the remaining flaps achieving closure; these dog ears disappear over time. If the wound is small, it can be allowed to heal spontaneously by contraction and epithelialization. Wounds smaller than 1 cm can heal spontaneously in a reasonable amount of time. Larger wounds may require a skin graft to heal quicker. Split-thickness grafts can be used for the benefit of wound contraction to result in a smaller area on the tip, which is not normal pulp.
Regarding the treatment of the bone in a digital amputation, the bone under the stump end must be smooth. Remaining bone chips and devitalized bone should be removed. The bone at the stump end can be smoothed by using a rongeur and file. Bone length is not as important as a stump with mobile nonsensitive coverage. The bone of the distal phalanx must be of adequate length to support the nail bed and nail growth (Ennis, 1938; Raitliff, 1969; Thompson, 1963; Chase, 1960). With digital amputations involving the thumb, length is important.
The articular cartilage can be preserved when the amputation occurs at the level of the interphalangeal joint. This articular cartilage can provide a shock pad for trauma and potentially causes less pain under than skin than the bone edges. Whitaker and Graham clinically evaluated the preservation of the articular cartilage with digital amputations and found a better outcome leaving the cartilage on the stump end (Whitaker, 1972). The protruding condyles and anterior aspect of the phalanx may be trimmed to provide a less bulbous stump.
In addressing the nerve at the stump end, it is important to avoid neuroma formation in this location. The nerve end should be in a position away from the stump end or an anticipated point of contact pressure. To minimize the risk for neuroma formation at the stump end, traction neurectomy of the digital nerve should be performed bilaterally for each digital amputation. The nerve is longitudinally distracted in the distal direction and then transected to allow for proximal retraction, leaving the nerve end 1-1.5 cm from the fingertip.
Preservation of a tendon insertion improves the active mobility and function of an amputation stump. Therefore, when possible, tendon insertions should be preserved. However, often the amputation level is proximal to the tendon insertion. The profundus tendon should never be sutured over the bone end or to the extensor because this can result in the quadriga effect. The quadriga effect results in less excursion of adjacent normal fingers because of the common profundus muscle from which all the profundus tendons originate. The amputated finger, which has a tighter profundus tendon, reaches the palm before the other fingers do and results in a weaker grip.
Another complication of tendon imbalance is the lumbrical plus posture, which is the paradoxical extension of the involved finger proximal interphalangeal joint with attempted flexion. This occurs when the profundus tendon is allowed to retract proximally, resulting in a pull on the lumbrical muscle as it originates from the profundus. The lumbricals contribute to metacarpal phalangeal joint flexion and interphalangeal joint extension. This proximal pulling of the profundus pulls the lumbrical tighter to extend the interphalangeal joints paradoxically with attempted flexion (Parkes, 1970). However, this lumbrical plus posture after amputations of the distal interphalangeal joint is rare. Also, adhesions can result; therefore, early motion of the amputated finger is recommended.
The digital arteries should be identified and ligated with small caliber sutures or be cauterized. The visible veins can be cauterized as well. Then the skin is loosely approximated to make sure there is no tension on the skin edges. If there is tension on the skin, the bone may be shortened or local flaps can be used.
When amputations are at the level of the distal phalanx, preservation of the profundus insertion is critical. An intact profundus improves functional contribution of the amputated finger and improves grip strength by providing active flexion at the distal interphalangeal joints in conjunction with the other fingers. Preservation of enough bone to support normal nail growth is perhaps the most crucial predictor of functional length with amputations at this level.
Amputations at the level of the distal interphalangeal joint can be closed over the articular surface of the middle phalanx. Local flaps can be used to provide soft tissue for closure over the middle phalanx if needed. The volar V-Y flap is the standard local flap option for injuries at this level. The volar V-Y flap is fashioned with the apex of the V at the proximal interphalangeal crease. When amputations are through the middle phalanx, preserving the flexor digitorum superficialis insertion is desirable. The flexor digitorum superficialis tendon inserts on the middle third of the middle phalanx. Amputations proximal to the superficialis insertion leave the amputated finger without active motion control at the proximal interphalangeal joint level and only with active motion at the metacarpal phalangeal level.
Amputations at the proximal interphalangeal joint can be closed over the articular surface of the proximal phalanx as are amputations at the distal interphalangeal joint. Amputations at this level can still actively flex at the metacarpal phalangeal joint through the action of the intrinsic muscles. If the amputation is near the metacarpal phalangeal joint, especially in the long and ring fingers, dropping small objects because of the defect can be addressed with finger prosthesis or ray amputation, with or without transposition.
Ray amputations
Index finger ray amputations
The index finger is the most important digit other than the thumb. The index is the primary finger used with the pinch function. If length, sensation, and mobility of the index finger are inadequate, the patient bypasses the index finger to preferentially use the middle finger for pinch functions. In this circumstance, an index stump can impede the function of the middle finger and the overall function of the hand. This is the primary indication for a ray amputation of the index finger.
The level of amputation that makes the index finger a candidate for ray amputation is controversial. Ray amputation of the index finger should not be performed acutely for injuries distal to the metacarpal phalangeal joint unless the spare parts are needed for salvage of other digits, such as the thumb. The remaining index finger may be left during a trial period after the initial injury. If the stump impedes function, it can be converted to a ray amputation electively. However, conversion to a ray amputation can narrow the palm and result in loss of grip strength and pronation strength, justifying a trial with the shorter index finger for laborers.
Murray found that power grip, key pinch, and supination strength are diminished by approximately 20% of normal with index ray amputations (Murray, 1977). Pronation strength is diminished by 50% in the same group of patients. The cosmetic appearance of an index ray amputation is highly acceptable.
In performing an index ray amputation, a dorsal longitudinal incision over the index metacarpal is used in conjunction with a circumferential skin incision at the midproximal phalangeal level. The skin is intentionally left long distally to avoid deficiency that could result in a web space contracture (see Image 1).
The dorsal veins are ligated, and the extensor tendons are transected. The periosteum is scored, and the metacarpal base is transected. The dorsal interosseous and lumbrical muscle tendons are transected. Studies have shown no difference in pinch strength with dorsal interosseous transfer to the second dorsal interosseous muscle; therefore, this technique is not indicated (Murray, 1977). Then, the flexor tendons are divided. The digital arteries and nerves are divided distal to the branches to the palmar skin. Interrupted sutures are used for skin closure. The hand is dressed lightly to allow for early motion.
Middle and ring finger ray amputations
When the middle and ring fingers are amputated at a level near the metacarpal phalangeal level, small objects fall through this area created by the gap of the missing digit. Patients describe difficulty in retrieving change from their pockets. This can be corrected with a ray amputation. However, the loss in grip strength and pronation strength has to be considered before performing ray amputations for these central digits.
The principles of a central ray amputation include removal of the injured finger at the metacarpal base, correcting the rotational deformity, closing the space between the 2 adjacent unamputated fingers, and achieving a satisfactory appearance of the hand. Two techniques of central ray amputation have been described. One involves the transfer of the index finger ray onto the third metacarpal base for the middle finger, and the small finger is transferred to the ring metacarpal base (see Image 2). The other technique involves removing the involved finger at the metacarpal base (see Image 3). The disadvantages of the ray transfer procedure are the requirement for postoperative immobilization and the risk of nonunion. Therefore, the authors' preferred technique for central ray amputation does not involve ray transfer.
The technique of central ray amputation involves the use of a circumferential incision at the midproximal phalanx in conjunction with a dorsal longitudinal incision (see Images 4-18). The dorsal incision is extended through the extensor. The periosteum is scored at the level of the metacarpal base. The metacarpal is transected at its base. Then, the hand is supinated, and the flexor is divided. The neurovascular bundles are divided proximally to avoid neuroma formation at the skin incision. The deep transverse metacarpal ligaments are identified on either side of the volar plate of the involved finger at the metacarpal phalangeal joint.
In transecting the deep transverse metacarpal ligaments, it is essential to preserve enough to attach to each other to minimize gap formation and rotational deformity. Then the ray is amputated. The gap is compressed, and transverse Kirschner (K)–wires are placed through the metacarpals on either side of the ray amputation. Threaded K-wires can help resist sliding of the metacarpals on the K-wires like an accordion. Then, the deep transverse metacarpal ligaments are repaired with 2-0 Ethibond nonabsorbable sutures. The threaded K-wire can help prevent rotational deformity. Active motion is begun early, and the K-wires can be removed at 6 weeks. This technique can be applied to ray amputation of both the middle and the ring fingers (see Image 19). Incomplete closure of the defect and scissoring must be carefully avoided with this technique.
Small finger ray amputations
The small finger plays a role in gripping and hooking objects. Small finger injuries are the most difficult to rehabilitate, and the finger often becomes stiff and immobile, possibly hindering hand function by catching on pockets or other objects. In this circumstance, small finger amputation can be considered. In a laborer, the amputation can be performed at the metacarpal phalangeal joint to remove the flail segment of the proximal phalanx but preserve a broad palm.
If grip strength is not a concern, a more esthetic appearance can be obtained with a small finger ray amputation. In performing a small finger ray amputation, it is important to preserve the insertion of the extensor carpi ulnaris, which inserts on the base of the fifth metacarpal (Swanson, 1964). This procedure is performed through a tennis racquet incision (see Image 20). Moreover, the hypothenar muscles are preserved to cover the gap and provide padding to the ulnar side of the hand (Louis, 1980.
Thumb amputations
The most critical digit to hand function is the thumb. Amputations of the thumb can be debilitating. The level of amputation determines the significance of the functional deficit. In general, the thumb is important as a post to which the fingers oppose. Therefore, in contradistinction to the length of the fingers, the length of the thumb is more important than active motion.
When the thumb tip has been amputated, replantation can provide the patient with the best return to function, even if interphalangeal joint fusion is required. In the event that replantation cannot be performed or is unsuccessful, minimal bone shortening should be performed to provide a smooth bone end over which to close the skin. In fact, the bone should not be removed only to obtain primary skin closure.
A volar rectangular advancement flap (Moberg) should be used to provide soft tissue closure and preserve thumb length (see Images 21-22). The volar advancement flap is raised as a rectangle to include both neurovascular bundles to the metacarpal phalangeal crease of the thumb proximally and is advanced in the distal direction. The Moberg flap can be used to close 1- to 1.5-cm defects (see Image 23). If the amputation level is at or distal to the distal interphalangeal joint, the patient should not experience much functional loss (see Images 24-25). If the patient's amputation level is proximal to the interphalangeal joint, reconstruction with toe transfer or metacarpal lengthening and web space deepening should be considered. If the amputation is at the carpal metacarpal level, pollicization can be considered if the index finger is not injured.
Transcarpal amputations
Transcarpal amputations are rare. Usually, amputations at this level can be replanted and an acceptable return of function is expected. When replantation is unsuccessful or cannot be performed, minimal reconstructive options exist for amputations through the carpus. In general, patients can be fitted with hand prostheses, which provide good cosmetic results. When the wrist supplies active motion, the prosthesis can be operated without an attachment to the elbow or shoulder harness.
Wrist disarticulations
Again, amputations at this level are rare and often can be replanted. Historically, amputations at the below-elbow level have been favored over wrist disarticulations because of the difficulty in wrist prostheses. However, with advances in technology, amputations at this level can be considered. Also, wrist disarticulation level is preferable in children compared to disarticulation below the elbow to preserve growth potential. The advantage of preserving the distal radioulnar joint is that full active pronation and supination can improve the function of the amputated appendage. Therefore, when possible, the distal radioulnar joint should be preserved. Also, the radial styloid flare should be preserved to improve prosthetic suspension. If possible, the palmar skin should be used to cover the stump end to provide thicker and more durable coverage.
Below-elbow amputations
In general, below-elbow amputations should be performed to preserve as much length as possible to preserve maximum pronation and supination. When traumatic amputations are more proximal, even 2 cm of ulnar bone length is sufficient to fit a below-elbow prosthesis. With more proximal amputations, the biceps can be reattached to the ulna at a position that approximates the normal resting length of the muscle. If the biceps is reattached under too much tension, a flexion contracture can result. A soft tissue deficit may require the use of a free flap or local flap to preserve the elbow (Jones, 1994).
Krukenberg procedure
The Krukenberg procedure is mentioned mainly for historical purposes. This operation was first described by Krukenberg in 1917. This procedure involves separating the ulna and radius for below-elbow amputations to provide a pincerlike grasp that is motored by the pronator teres muscle. The indication for this operation is reserved for a blind person undergoing bilateral amputation because it can provide prehension and tactile gnosis.
Elbow disarticulations
Elbow disarticulations are preferred by surgeons and prosthetists over above-elbow amputations because they allow for rotary force transmission over the humerus and the epicondyles provide good support for the prosthesis. The disadvantage of an amputation at this level is that the prosthesis has outside locking hinges, which can damage clothing.
Above-elbow amputations
In traumatic above-elbow amputations, bone resection should be avoided because maintenance of stump length is critical to function. The longer humeral stump has better proximal muscular control and provides a long lever to help maneuver the prosthesis. Even if required for primary closure, bone shortening should be avoided. Split-thickness skin grafting can be considered over the stump end to preserve stump length. It is essential to have bone below the insertion of the pectoralis major. Amputations that are more proximal to the pectoralis are essentially shoulder disarticulations because shoulder motion is lost.
posted by Mr.O&P Student at 8:25 PM 0 comments
Prosthetic Options for the Lower-Limb Amputee Including Immediate and Early Fittings

Figure 1
By Donald Shurr, CPO, PT
In 1922, Wilson reported using plaster casts fitted with wooden or metal pylons for early ambulation. Berlemont, in France and Weiss later in Poland, and Burgess in the United States, reported using this system; only these were applied in the operating room immediately following the surgical procedure. These systems allowed for early weight bearing and quicker time to final prosthesis, as reported by numerous authors. A careful review of these papers reveals most to be anecdotal, but the enthusiasm spread throughout the prosthetic community.
The literature reported several objectives accomplished by the use of these systems. Most of the early systems provided some degree of protection to the fresh wound. Falls were common and remain so today. The thigh-level systems, whether plaster, fiberglass, or later thermoplastics, prevent knee-flexion contractures.

Figure 2
Systems allowing for the attachment of a pylon and prosthetic foot can allow patients to walk partial weight bearing as early as postoperative day two, depending on physician preference, wound status, and other potential complicating factors such as diabetes. The APOPPS™ (Adjustable Post-Operative and Preparatory Prosthetic System) (see figure 1), by FLO-TECH® O&P Systems, Inc. consists of the FLO-TECH-TOR™, which provides protection from trauma caused by scrapes and impact injuries and flexion contractures until the wound heals, the VCSPS™ (preparatory socket), and the UFOS™ (Universal Frame Outer Socket), which accepts both the protective and the preparatory sockets and allows for the attachment of pylon and prosthetic foot components.
Once the wound is healing and the surgeon or managing physician recommends early weight bearing, the Rehab System (FLO-TECH-TOR™ and UFOS™) or the Prep System (VCSPS™ and UFOS™) may be employed. These systems consist of a flexible thermoplastic inner socket (FLO-TECH-TOR™ and VCSPS™) and a more rigid thermoplastic outer socket (UFOS™) (see figure 2).
Other systems available to the certified prosthetist include those made of air bladders as well as the traditional wrap casts and pylons. An advantage of these latter systems is that they are not easily removed by the patient. Lew Schon, MD, has published very detailed reports of the bladder systems and their positive results on many patients with diabetes, using prefabricated prostheses in a prospective study.

Figure 3
As with many other patient care techniques used by prosthetists and orthotists, careful attention to detail often spells the difference between success and failure. Close communication with managing physicians is also important so that each can bring his or her expertise to a successful outcome for the patient.
A second group of patients, albeit a smaller number, with similar needs are those who undergo a transfemoral amputation. Unlike the transtibial amputee, fewer options exist for this group. In our hands these systems are used for the patient with an amputation secondary to a bone or soft tissue tumor and for whom all other options have been rejected. These patients have both length and circumferential differences, making conventional sockets difficult, especially in the early weeks following surgery. This group of patients can ambulate using a partial weight bearing limitation as the prosthesis allows for a safer and less energy costly gait.
FLO-TECH® has a companion system for patients at the transfemoral level, the complete APOPPS-TF™ system. It offers the same protection, adjustability, and weight bearing capability as the TT version. And using the endoskeletal system allows the knees to be substituted as many of this group may be more active than older, dysvascular amputees of the same anatomical level (see figure 3).
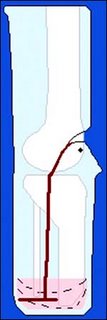
Figure 4
The APOPPS™ and the APOPPS-TF™ allow the surgeon to inspect the wound healing daily and the patient to begin walking on day two. Properly instructed patients report an advantage of the FLO-TECH® system is that by simply adjusting the straps and bands on the socket they (the patients) usually do not feel the need to remove the system. As healing occurs, socket modification is done using circumferential straps to tighten the socket, and the addition of stump socks offsets atrophy and volume changes. The VCSPS™ and APOPPS-TF™ are adjustable in AP, ML, and circumference at all levels and as such may provide optimum comfort without the need for additional stump socks, although the cushioning provided by adding more stump socks is a comfort option. Both TT and TF systems are designed with suspension systems to reduce the chance of pistoning and the friction that goes with it. One should expect more pistoning during the early stages of ambulation with the FLO-TECH-TOR™ and the APOPPSTF ™, as these sockets are designed so as not to adversely resist distal migration (see figure 4). The distal pads used in the socket are lively and will return to their original shape immediately after pressure is removed; thus the pads maintain distal contact at all times, prevent pooling of edema distally and promote healing. The pylons used are endoskeletal, allowing the length, tilts, change of components and alignment to be adjustable throughout the life of the system.
FLO-TECH® provides custom fabrication of standard, ischial weight bearing, Symes, knee disarticulation, youth and children’s sockets and systems.
Anyone using these or other systems would be well advised to review the supplement to the Journal of Prosthetics and Orthotics (JPO), Volume 16, Number 3, July 2004. This is the official finding of the consensus conference on Post-Operative Management of the Lower Extremity Amputee published by the American Academy of Orthotists and Prosthetists.
 OK ... cutting your leg off is truly an experience ... but one that you can survive. It would seem that dealing with your insurance provider is the greater challenge. If you are struggling with your coverage, the two C-Leg Appeals written to Humana might be of help to you! The first was required to convince them to provide a microprocessor knee ... the second was necessary because of all the needed steps they denied on their response to my first appeal.
OK ... cutting your leg off is truly an experience ... but one that you can survive. It would seem that dealing with your insurance provider is the greater challenge. If you are struggling with your coverage, the two C-Leg Appeals written to Humana might be of help to you! The first was required to convince them to provide a microprocessor knee ... the second was necessary because of all the needed steps they denied on their response to my first appeal.






